
A humanitarian crisis. Hospitals lacking available beds. Devastated by underemployment. These recent findings perfectly encapsulate the position our healthcare is in.
In light of the current crisis in the NHS, we felt it correct to follow our education skills shortage piece with one looking at the struggles of the health sector in the UK.
From nurses, to medical radiographers, the sector is suffering from staff shortages. But just how bad is this? How can the Department of Health, Health Education England (HEE), and the various trusts reverse the fortunes of the health industry?
Evidence of staff shortages in the health sector
From the cradle to the grave.
That was the promise made when the NHS was formed in the aftermath of World War Two. It’s something we still rely on heavily to this day, and probably sometimes take for granted.
However, we should all be worried at its long term effectiveness, given the staffing challenges that exist.
In their ‘Managing the supply of NHS clinical staff in England’ document, the National Audit Office (NAO) document many concerning findings:
- A 5.9% shortfall in staff in 2014, equivalent to 50,000 clinical staff.
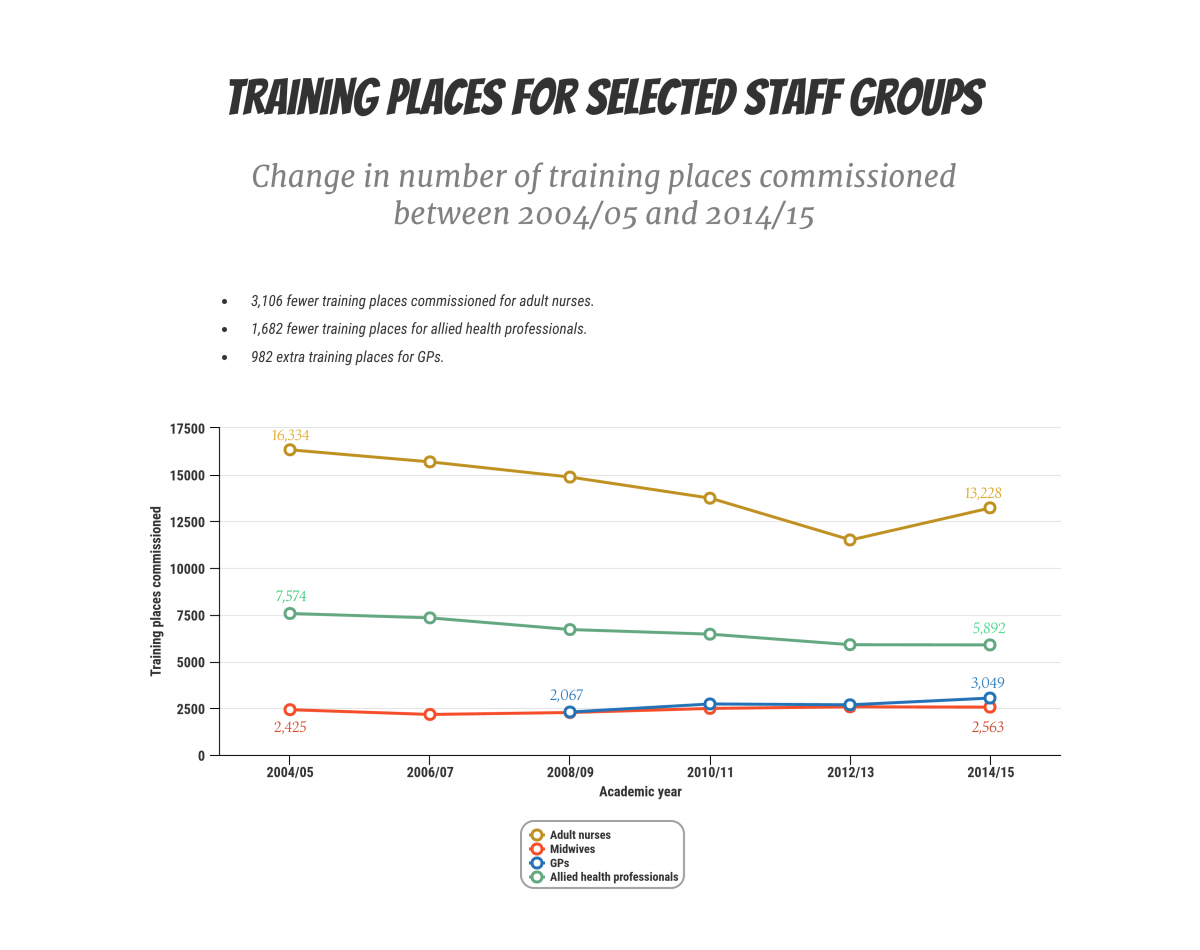
- In the 10 years since 2004 / 05, there have been 19% fewer training places for nurses.
- 61% of all temporary staffing requests were to cover existing vacancies in 2014 / 15.
- Fewer clinical staff returning to work.
Among the most disconcerting issues brought up in the document is the fact that the number of nurses leaving the NHS has increased from 6.9% in 2010 / 11 to 9.2% five years later.
Recruitment of new GPs and nurses remain low while population in England steadily increases. As currently delivered, the system seems to be approaching saturation point.
This is compounded by instances of non clinical staff leaving the profession has also increased from 7.9% to 9% in the same time period.
Ensuring there are enough GPs is also a challenge, according to the NAO’s ‘Improving patient access to general practice’ paper. This shows evidence that the proportion of GPs leaving the profession is steadily rising.
The number of GPs between 55 and 64 who have left the profession doubled between 2005 and 2014.
Supply not meeting demand
There’s no doubting the efforts to increase the number of healthcare staff, both to replace those leaving the industry, and to keep pace with the demand.
Between 2004 and 2014, NHS clinical staff increased by 1.4% each year on average.
Health Secretary, Jeremy Hunt, said in the Commons that in the past six years, the number of people over 80 has increased by 340,000 and life expectancy has gone up by 12 months.
However, the brutal truth is the supply of NHS clinical staff does not currently match demand.
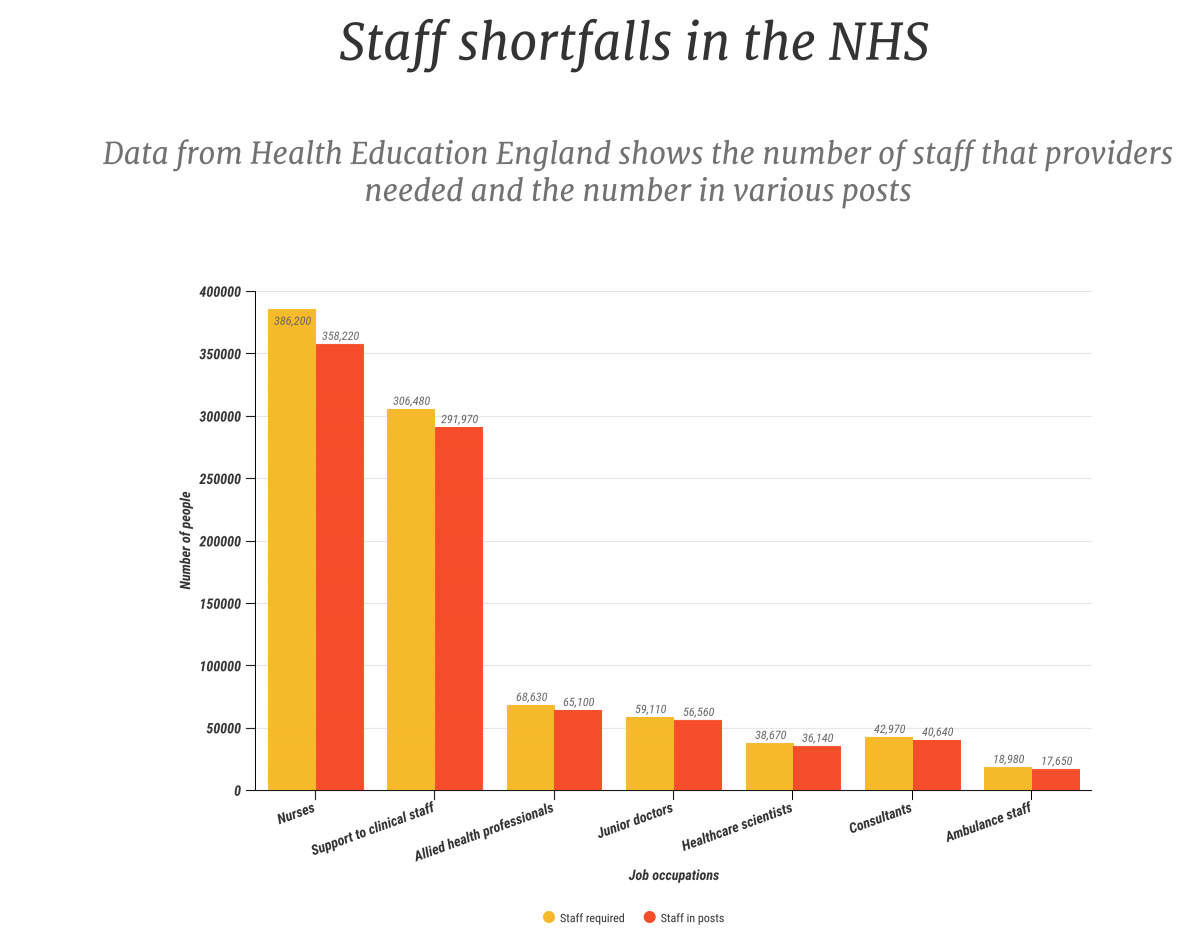
In figures gathered by HEE in 2014 for instance, every single staffing profession suffered from a shortfall.
The biggest percentage was for nursing, midwifery and health visiting staff – 7.2% down on the number of employees needed.
Ambulance staff (7%), healthcare scientists (6.5%) and consultants (5.4%) don’t fare much better.
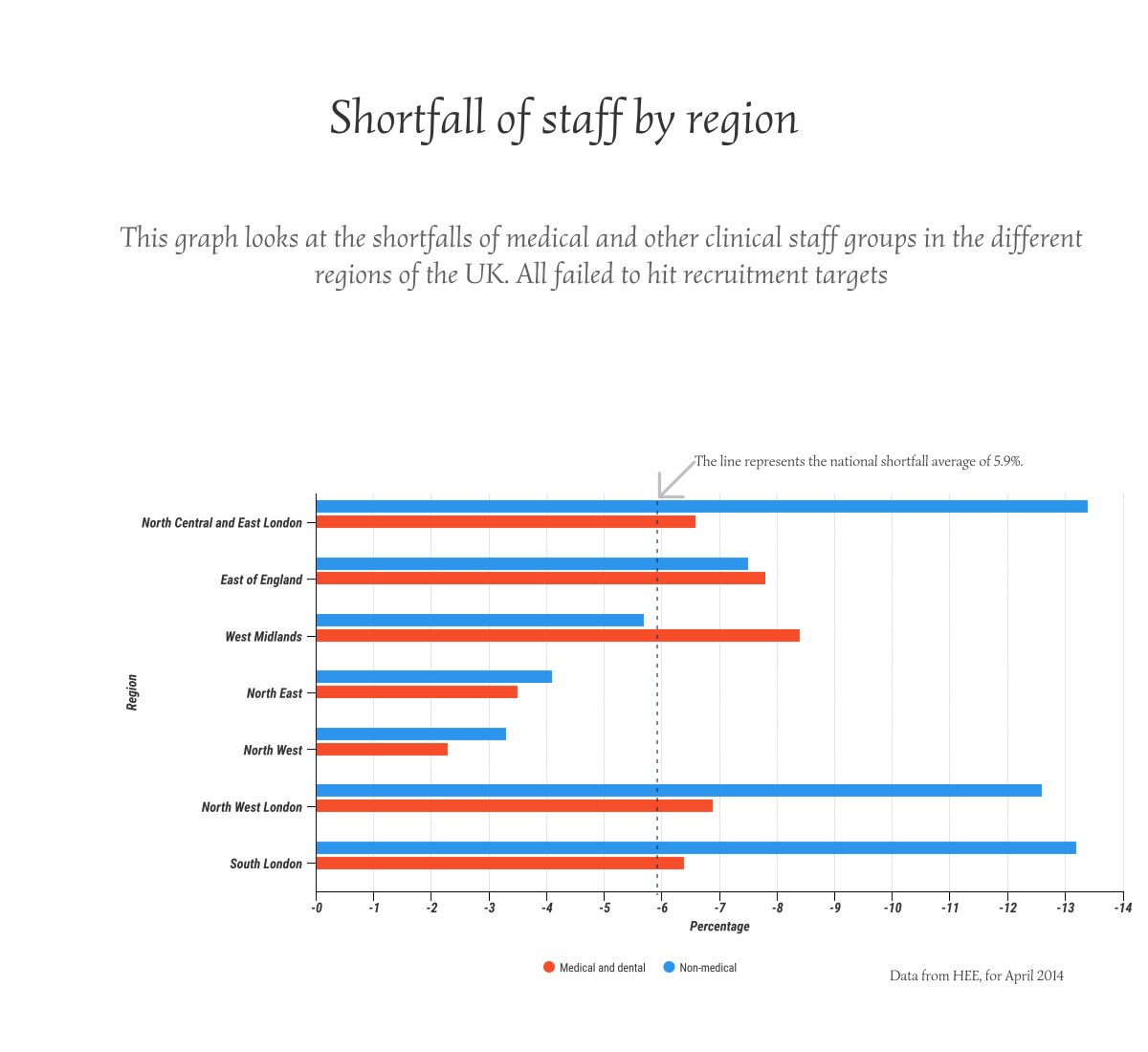
The extent of staffing shortfalls vary wildly depending on the region of the country. Some of the shortfalls are discernibly less than the national average of 5.9%, while some – like North Central and East London – are much higher.
Regardless of region, all are suffering from medical and non-medical staff shortages.
Why are we suffering from health skills shortages?
There isn’t just one reason why the industry is in crisis. Just weeks ago, the extent was laid bare by the news that, in the run up to Christmas, 50 of the 152 English trusts were at their highest or second highest levels of pressure.
We have an increasingly ageing population, with longer life expectancy and increased incidence of co-morbidity, so demand on health and care services is increasing.
The University of Derby has several partners that provide care and their Dean of the College of Health and Social Care, Paula Holt, said that these NHS partners and care providers “are experiencing shortages of most healthcare professionals including nurses, doctors, radiographers and therapists.”
However, there are factors alongside lack of staff that are contributing to the overall problem.
An analysis of GP and nurse consultations last year by researchers from the universities of Oxford and Bristol, highlighted an imperfect storm of factors that are combining to severely hamper the NHS.
Professor Richard Hobbs, lead author from the Nuffield Department of Primary Care and Health Sciences at the University of Oxford, explains:
“The demands on general practice have increased substantially over the past seven years. Recruitment of new GPs and nurses remain low while population in England steadily increases. As currently delivered, the system seems to be approaching saturation point.”
At a time when demand for staff is increasing, there are signs that the pressures are leading to demoralised employees turning their backs on the industry.
Healthcare recruitment agencies are also feeling the strain, with 1 Stop Healthcare seeing “significant rises in demand for healthcare professionals.”
Clare Sanderson, Sales and Operations Director attributed this to more than one reason.
“With increased population and health complexities throughout the UK, the need for our services is constantly in demand for both learning disability and older person care.”
What reasons have contributed to today’s shortage?
Rise in population and patients
It is true that we have a shortage of clinical staff in the UK but this is being exacerbated by the increase in population and life expectancy.
Health Secretary, Jeremy Hunt, said in the Commons that in the past six years, the number of people over 80 has increased by 340,000 and life expectancy has gone up by 12 months.
The number of GPs between 55 and 64 who have left the profession has doubled between 2005 and 2014.
Medicine has also come a long way in the last 50 years, with breakthroughs finding cures and prevention for some diseases while helping people live longer with others.
While this is great for us and our loved ones, it puts into sharp focus the relative lack of doctors, nurses, consultants and other medical professionals needed.
Paula Holt at the University of Derby highlighted this as one of the main reasons for the skills shortage in healthcare.
“We have an increasingly ageing population, with longer life expectancy and increased incidence of co-morbidity, so demand on health and care services is increasing.”
Underemployment and higher workloads lead to people leaving profession
This winter has shown just how grave the situation is in the NHS, with medical practitioners throughout the country expressing how the industry is devastated by underemployment and threatened further with the real possibility even more will leave.
NHS plans to recruit an additional 5,000 GPs will take some time and crucially, depend on an improved appeal of general practice as a career choice.
Patient numbers are increasing, therefore hospitals and ambulances are finding it impossible to keep up with demand.
These concerns are not new, and the warning signs have been there for some time.
Findings published last April – based on analysis of more than 100 million GP and nurse consultations between 2007 and 2014 – showed that workloads increased by 16%.
Adults over 85 had some of the highest consultation rates; showing that the ageing population is increasing demands that aren’t being met.
And although there has been a rise in the number of GPs during this time, the sheer volume of consultations means there has been a decrease in the number of GPs per patient.
At a time when demand for staff is increasing, there are signs that the pressures are leading to demoralised employees turning their backs on the industry.
All NHS trusts are under pressure to deliver a successful and sustainable service, but NAO findings said plans appear to be influenced as much by meeting efficiency targets as by staffing needs.
Nobody can be under any illusions at just how stressful this type of work is – GPs, consultants and nurses have people’s lives in their hands on a daily basis.
Poor morale and stress are key factors in GPs leaving their profession and although measures were set out last year to improve workload in general practice, 69% of GPs rated this support as ‘poor’.
Nurses are also leaving the health service at an alarming rate. In 2014, 5.7% of nurses yet to reach retirement age left the NHS.
In this context, a career in healthcare isn’t attractive, and Professor Hobbs believes this needs to improve.
“NHS plans to recruit an additional 5,000 GPs will take some time and crucially, depend on an improved appeal of general practice as a career choice.”
Social care shortages
As the average age of the population rises, so too does the need for social care. Again, this is an industry that is suffering from shortages.
Commissioning training places correctly is key to long term success; not only to ensure that staffing levels are adequate, but to guarantee that money is not wasted.
Much like GPs, nurses and other clinical staff, workload pressures are apparent.
Many elderly people understandably choose to receive care at home. However, according to Barry Sweetbaum, founder of SweetTree Home Care Services, this leads to higher workloads for employees who don’t earn a great deal.
“Due to the very low fees paid to providers in relation to the care delivered, those working in the community are generally paid at minimum wage, put under great pressure to go from client to client, regardless of whether or not they have been allocated enough time to do all that is required of them.
“In circumstances such as this, carers feel stressed, undervalued and disillusioned with their role, and consequently choose to work elsewhere.”
Staff recruitment requirements and financial requirements?
Cost of employing enough staff to meet demand for healthcare has significant impact on providers’ financial position and sustainability.
Perhaps this is the main reason behind staff shortages: The financial pressures of balancing the books while trying to recruit employees.
All NHS trusts are under pressure to deliver a successful and sustainable service, but NAO findings said “plans appear to be influenced as much by meeting efficiency targets as by staffing needs.”
The findings show that this focus on efficiency has lead to HEE not commissioning enough places to train staff in.
Because of this, significant gaps in staffing can develop and therefore, eat into money in order to finance this shortfall.
The gaps in staffing and financial difficulties all look part of a vicious cycle; hospital trusts have to call on temporary staff to plug these gaps, but this is inefficient as well as expensive.
Nurses are also leaving the health service at an alarming rate. In 2014, 5.7% of nurses yet to reach retirement age left the NHS.
More concerning is the fact that in 2014 / 15, 61% of temporary staffing requests were for unfilled permanent vacancies.
To be clear, temporary staff provided by agencies are of great importance to the NHS. They help to fill gaps when trusts are short staffed for anything like holidays or sickness. Indeed, there are 400 agencies listed by NHS Employers as providers.
However, when more than half of requested temps are to fill permanent vacancies, it’s clear something is wrong with recruitment and the financing of this.
More has to be done to secure permanent staff members, otherwise hospitals and doctors’ surgeries won’t be able to cope in the long term.
How can the skills shortage be averted?
Better collaboration at a national and local level would benefit the industry when plans are put in place to forecast staff requirements.
As it stands, local education and training boards are responsible for producing regional workforce plans, which leads to the HEE producing a national plan by aggregating those at the regional level.
Our numbers are too low, and at present we need the support of European nurses who might otherwise be attracted to work in Germany or the Scandinavian countries.
However, the system is flawed because it doesn’t take into account the differentials that will undoubtedly exist at different localities – none are the same after all – while the supply and demand model isn’t comprehensive.
Another issue to consider at the regional level is whether these plans can take into account the intention to change the way services are delivered – such as providing more care outside hospitals, and the prospect of a seven-day NHS.
More trainee places for health sector jobs
We have seen that shortfalls exist in all professions. From ambulance staff to junior doctors, not enough are being recruited.
There are a number of ways staff numbers can be boosted but a long term approach has to be maximising the use of training.
Commissioning training places correctly is key to long term success; not only to ensure that staffing levels are adequate, but to guarantee that money is not wasted.
The latest NAO document showed that 3,019 GP training places were filled in 2016 / 17 – 93% of the target amount.
For example, the estimated training cost for one nurse is £79,000, and it takes three years before they fully qualify.
GPs meanwhile, cost in the region of £485,000 for their 10 years of training, and each consultant has 14 years of training at a cost of £727,000 per person.
Forecasting staff is difficult because of how the need for services can change in a decade, but it is vital that the methods in place give the best possible estimate, otherwise the above financial outlays could be wasted halfway down the line.
Looking at the figures, a rise of almost £5 billion for education and training between 2006 / 07 and 2014 / 15 seems positive, but this is less as a proportion of overall health spending.
Each year, the HEE commissions 130 education and training programmes, meaning there are approximately 140,000 students training at any one time.
Funding for schemes to support nurses returning to the NHS costs £2,000 – a huge difference to starting training from scratch.
However, for some professions, fewer training places were commissioned in 2014 / 15 than in 2006 / 07.
Shortfall in number of commissioned training places
The fall in training places, and failure to keep pace with demand suggests a shortage of prospective candidates.
However, Paula Holt at the University of Derby suggests the opposite is true:
“The number of nurses, midwives and allied health professionals we have been able to educate has been restricted by Health Education England via the commissioning process, despite NHS workforce plans stating we need more health and care professionals.
“There has been absolutely no shortage of applicants for these programmes – they are heavily applied for.”
What will help are the more innovative approaches to enhancing the workforce through new roles and routes to registration, such as the new Nursing Associate role, and degree apprenticeships for nursing.
Given the shortages, the fact there are people wanting to train but unable to do so is astounding and it’s clear that the Department of Health, the HEE and various trusts need to address this.
To their credit, some trusts are now funding their own training places to supplement the ones already commissioned – Lancashire Teaching Hospitals NHS Trust has a contract with the University of Bolton to train nurses.
The HEE is trying to reduce the number of people leaving training by 50%, and financial incentives have been made available, such as exemption from tuition fees for some professionals.
Clearly though, more is needed.
Even though universities can increase their student intake because of extra funding of loans, the Placement Tariff – which supports student placements – has not been increased. This is a mandatory part of healthcare education.
There has been absolutely no shortage of applicants for these programmes – they are heavily applied for.
According to the University of Derby’s Paula Holt, more places are needed on programmes that lead to registration as healthcare professionals, and all routes should be explored.
She said: “What will help are the more innovative approaches to enhancing the workforce through new roles and routes to registration, such as the new Nursing Associate role, and degree apprenticeships for nursing.”
Make use of return to work initiatives
The trend for temporary staff has increased in recent years, and the majority are now needed to cover unfilled vacancies.
In the five years to 2015, expenditure on temporary staff increased from £2.9 billion to £4.7 billion.
Many employees, including nurses, are leaving each year before retirement age, meaning there is a resource here of fully qualified professionals who should be targeted to fill the gaps.
With Brexit looming, this may seem like a doom and gloom scenario, but the reality is many foreign nurses still value the training and sharing of skills and knowledge, as well as the exciting lifestyle afforded within the UK.
In recent years, the focus on return to work practices hasn’t been as strong as it was. 18,500 former midwives and nurses completed return to work courses between 1999 and 2004. This number was cut by three quarters between 2010 – 2014.
It’s a viable option that should be explored because, amongst other reasons, it provides:
- Value for money.
- Reduce temporary staffing costs.
- Experienced employees ready to step straight into hospital work.
Funding for schemes to support nurses returning to the NHS costs £2,000 per person – a huge difference to starting training from scratch.

Bridging the skills gap in healthcare is proving to be a growing problem.
In addition, approximately 80% of those who complete courses return to nursing.
They are then employed by the trust in question, meaning those who trained these nurses benefit from their employment, rather than lose them to others, therefore easing local staffing pressures.
Recruiting GPs from overseas
The latest NAO document showed that 3,019 GP training places were filled in 2016 / 17 – 93% of the target amount.
The number of nurses, midwives and allied health professionals we have been able to educate has been restricted by Health Education England via the commissioning process.
Despite targeting 5,000 extra doctors by 2020, the profession is at risk from falling retention levels too, so all avenues to source staff are urgently required.
Recruitment from overseas would be much easier if GPs were on the shortage occupation list, however NHS England failed to secure this.
Instead, the General Practice Forward View from April 2016 included intentions, for an international recruitment campaign.
How this pans out in light of the EU referendum is anybody’s guess but if the HEE is to arrest the shortages, action needs to be taken.
Last month provided some respite, as Lincolnshire LMC recruited its first wave of international GPs from Europe, who will start training in Poland this month.
Better collaboration at a national and local level would benefit the industry when plans are put in place to forecast staff requirements.
It is part of a pilot initiative that NHS England chose Lincolnshire for, which will see the arrival of 25 recruits by August.
Rolling this out on a wider basis will go some way to meeting the target of 500 GPs from overseas.
Recruitment of overseas nurses
Recruitment of nurses from overseas is down as well: less than 8,000 were added to the Nursing and Midwifery council register in 2014 / 15 – a decrease of 4,000.
The number of nurses recruited from Europe in the last 10 years has increased but Tony Moss, CEO and founder of global recruitment agency Your World Healthcare, believes the UK needs to target these employees.
Among the most disconcerting issues brought up in the document is the fact that nurses leaving the NHS has increased from 6.9% in 2010 / 11 to 9.2% five years later.
He said: “Our numbers are too low, and at present we need the support of European nurses who might otherwise be attracted to work in Germany or the Scandinavian countries.
“With Brexit looming, this may seem like a doom and gloom scenario, but the reality is many foreign nurses still value the training and sharing of skills and knowledge, as well as the exciting lifestyle afforded within the UK. This is not set to change.”
How can the health skills shortage be averted?
There’s no quick fix or easy solution. The shortages in staff levels are worse because of the crisis engulfing the health sector, which is putting more strain on the industry than ever.
The trusts, Department of Health and the HEE all need to maximise the various routes available to recruit staff. This is the only way to fight against shortages, stem the flow of those leaving, and tackle the ever-increasing patient numbers.
All of these organisations simply must do whatever is necessary to remind current and prospective employees that a career in healthcare is an attractive option.
It is imperative if we are to have a functioning health service in the long term.